Lessons Learned

Hindsight is 20/20, but it rarely helps to predict the future — except in the world of incident analysis. Introspective analysis is one of the strongest tools that we have as a community to improve dive safety. By analyzing the incidents that occur to divers, we can effectively tend to dive injuries and respond to real incidents occurring across the globe.
For three decades the researchers at DAN have monitored, tracked and analyzed diving incidents and fatalities worldwide. One of the best sources of this incident data is you, the diver. When you self-report an injury or incident that you experienced or witnessed via the DAN Incident Reporting System, you offer a valuable look at real world diving incidents and injuries.
For this issue of X-Ray Mag, we wanted to share this incident from an extremely experienced CCR diver who developed immersion pulmonary edema (IPE) at nearly 300 FSW. While we may not all be able to perform that dive ourselves, it is entirely possible that we could suffer similar symptoms at much shallower depths, and we can prepare ourselves to respond to symptoms of IPE by learning how she handled her incident. Read this divers story, and use it to keep yourself safe in the water this winter.
Diver Incident Report Synopsis:
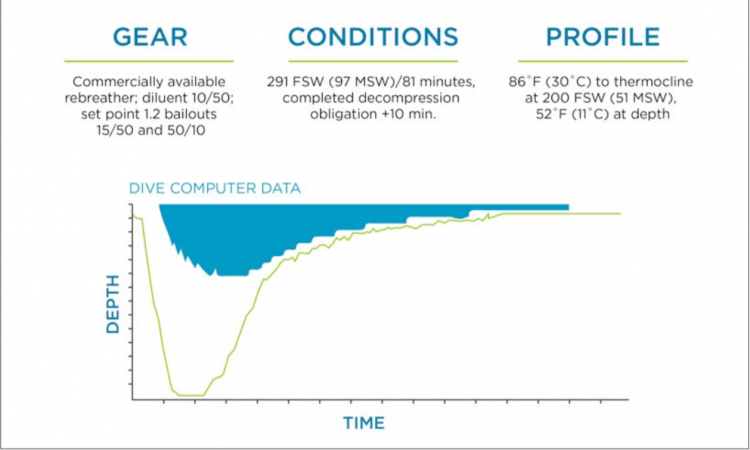
With cold conditions reported on the bottom, this diver borrowed a 5mm wetsuit and hood to replace the 3mm wetsuit she had initially intended to use. Her buddy wore a drysuit. Both divers were using closed circuit rebreathers, and carry two open circuit bailouts containing 15/50, and 50/10. The planned dive was a 10-15 minute bottom time at 291 FSW with a direct descent, and free ascent.
The initial descent was uneventful, with a thermocline noted at 186 FSW, and a bottom tempera- ture of 52oF. The dive plan was to swim along the bottom until one diver became too cold, and then ascend. After a few minutes at depth, this diver reported feeling a tickle in her throat and coughing a few times. The diver then coughed once or twice a minute for about ten minutes. Coughing is abnormal for this individual, who is an endurance triathlete and in excellent physical shape. After approximately 10 minutes, coughing worsened and the diver reported feeling like she was working and breathing hard. At this point, the diver also began to feel cold and signaled her buddy to ascend.
During the ascent, at approximately 200 FSW, the diver experienced a gurgling noise upon inhalation, and reported that it felt like she was gargling water right behind her Adam’s apple. In addition, the coughing continued. At this point in the dive, both the diver and her buddy had 52 minutes of decompression remaining, and the diver decided to minimize exercise and finish as much of that decompression as possible before symptoms could worsen and force an ascent.
At their first decompression stop around 90 FSW, the divers ascended into warmer 86°F water. The coughing and gurgling symptoms continued, and by the time the diver had reached her 70 FSW stop she was having a difficult time breathing and felt like she was overheated. Too task-loaded to take it off, the diver cut off her hood with scissors to remedy the situation, and continued to minimize movement and focus on her ability to breathe.
At 30 FSW, it became apparent that the diver's buddy did not know she was in trouble, and so the diver signaled that she was “badly bent” on a slate, and had the buddy deploy a yellow surface market buoy, a predetermined emergency signal that had been discussed with the charter boat crew. The crew responded by sending a safety diver into the water with a bottle of oxygen, which the diver refused for fear of compromising her buoyancy and making her exercise more.
The diver did manage to complete her decompression despite the coughing, and spent an additional 10 minutes at her last stop depth. Upon surfacing, the diver was removed from the water, stripped of her equipment, and placed on emergency oxygen while being transported in a waiting ambulance, and then to a local hospital. Symptoms did begin to improve upon surfacing, although they did not abate entirely. X-rays confirmed pul- monary edema, and the diver was kept for observation in the hospital overnight, and released the next day. The diver reports that the outcome was good, and there are no lingering issues. To read the diver's full report, visit:DAN.org/diving-incidents
DAN Expert Analysis:
This diver was experienced but improperly prepared for the thermal stress of the dive. The equipment improvisation may or may not have contributed to the event, but fit issues did add some discomfort as evidenced by actions taken during ascent. The diver was generally cool-headed and exercised good judgment in what would undoubtedly be a stressful situation. With the support of her buddy, she likely avoided a much more complicated outcome that would have arisen following an abbreviated or aborted decompression.
The key weakness in this case was likely communication, with contradictory messages leading to confusion for both the buddy and the surface team. Expecting some degree of confusion in any evolving case, the need for clear, ongoing and flexible communication is clear. Divers often focus on decompression stress, but it is important to remember that a variety of problems may arise.
Immersion pulmonary edema results from a combined effect of increased central blood volume and increased work of breathing. Central blood volume is increased by immersion, cold stress and possibly high levels of fluid intake. Work of breathing is increased by the breathing circuit, body position, gas density and physical exercise and stress. Problems are more likely to arise when multiple factors, possibly each modest individually, act together.
To report a diving incident, visit DAN.org/research/IncidentReport
For more information on IPE and diving, visit DAN.org/Health
- Log in to post comments




























































 is one of the conditions more likely to occur in technical and mixed-gas diving")

























")


 the flat-bottom and the Ses Fontanelles I.")








